
Promoting MMJ Among Pain Management Specialists in the USA
Marijuana Industry NewsMedical Marijuana May 9, 2019 MJ Shareholders 0
By John Taenzler, Ph.D.
Millions suffer from acute or chronic pain every year and the effects of pain exact a tremendous cost in terms health care costs, rehabilitation and lost worker productivity, as well as the emotional and financial burden it places on patients and their families. The costs of unrelieved pain can result in longer hospital stays, increased rates of rehospitalization, increased outpatient visits, and decreased ability to function fully leading to lost income and/or insurance coverage.
According to a recent Institute of Medicine Report, pain is a significant public health problem that costs society at least $560-$635 billion annually, an amount equal to about $2,000 per U.S. citizen.
Although there have been few clinical trials investigating the effect of marijuana on mediating pain, findings to-date support positive results. A study from Israel showed that of 322 patients with fibromyalgia using MMJ, 94% reported pain relief, 93% had improved sleep, 87% reported improvement in depression and 62% had reduced anxiety[1]. Further, an audit of 18 randomized clinical trials[2]focused on pain and MMJ showed positive outcomes for 16 of the trials when treating pain associated with neuropathy, spasms, post-operative pain, spinal injury, rheumatoid arthritis, cancer and urinary tract symptoms.
Ten years ago, a study conducted by the Institute of Medicine (IOM) recognized the role that cannabis can play in treating chronic pain: “After nausea and vomiting, chronic pain was the condition cited most often to the IOM study team as a medicinal use for marijuana.” These conclusions were based on more than 300 studies showing that cannabinoids and cannabis can provide relief to patients experiencing chronic pain. Further, the IOM report found that “basic biology indicates a role for cannabinoids in pain and control of movement, which is consistent with a possible therapeutic role in these areas. The evidence is relatively strong for the treatment of pain and intriguingly, although less well established, for movement disorder.”[3]
Despite these findings and with the recently sharp rise in opioid-related deaths, why are not more pain specialists turning to MMJ for their pain patients?
In October 2018, a survey was conducted among 86 pain management specialists (APMs) in 15 of the States where medical marijuana (MMJ) has been legalized and available. In examining and assessing the perceptions and attitudes of these APMs towards MMJ, physicians were asked about their current use of MMJ for their patients and given their current knowledge-base how likely they are to recommend MMJ in the future to pain patients. These questions were used to segment APMs based on their future willingness to recommend MMJ.
- Willing APMs (n=53)
- On-the-fence APMs (n=13)
- Unwilling APMs (n=20)
Current Use of MMJ
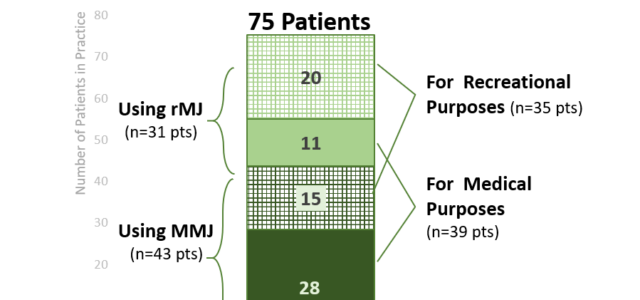
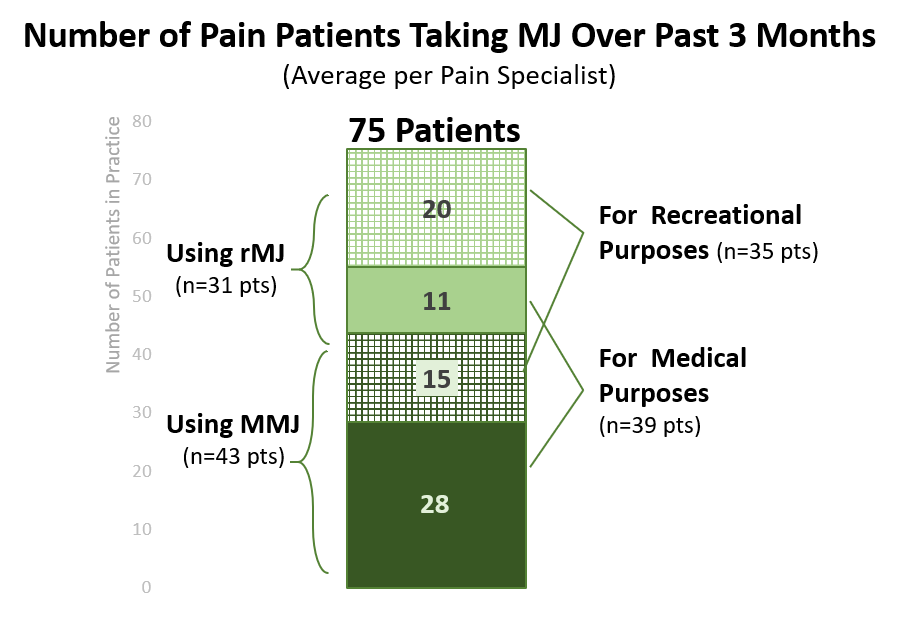
Overall, 38% of APMs in the USA say they currently recommend MMJ to their pain patients, 15% have done so in the past, but 47% have never recommended MMJ. This is despite over one-fourth (27%) of physicians’ patients taking an opioid, 70% of these patients using opioids on a daily basis, and 43% of these patients using opioids for 1 month or longer. On average, APMS in the U.S. estimate that they each have 75 patients using cannabis, with more than half (n=39) using it for a medical purpose.
As expected, APMs opposed to recommending MMJ to their pain patients are more likely to recommend against using MMJ (38% of enquiring patients) and are less likely to supply patients with written and/or verbal information about MMJ (21% of patients). This is opposed to APMs who are willing to advocate for MMJ (these APMs recommend against using MMJ to only 17% and provide info to 43% of patients).
Overall, when it comes to information about the impact of MMJ on pain, APMs, as a group, are most knowledgeable about the psychoactive properties of THC, with nearly 4 in 10 (38%) reporting familiarity with the topic. Conversely, few are familiar with the pharmacology of different aspects of cannabis including CBD (35% claim familiarity), THC (31%), CBN (30%), or terpenes (8%). As such, despite many of these APMs having patients report beneficial outcomes from using MMJ, a majority of these physicians doubt the true clinical impact of MMJ on pain.
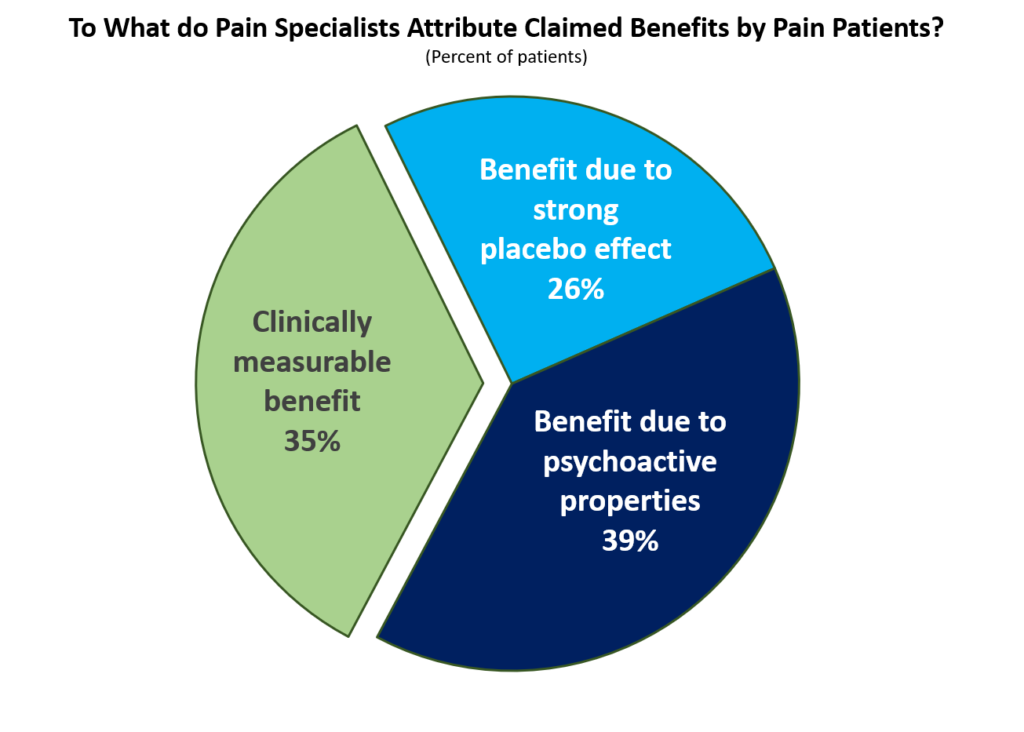
As shown in the chart below, only one-third (35%) say that the pain relief demonstrated a clinically measurable benefit. They say that most claims of pain relief are justified as being the result of a placebo effect or due to the patient being high.
APM Profiles
The APMs currently willing to recommend MMJ to their pain patients are significantly more familiar with many of the topics regarding cannabis than are APMs unwilling to recommend and those on-the-fence.
- Willing APMs are more familiar with many of the pharmacologytopics for MMJ, including: the classifications of cannabis, the pharmacology of THC and of ingestible forms.
- These APMs are also more familiar with logisticsin terms of where dispensaries are located and what types of ingestible forms are currently available.
- They are also more familiar with the anti-inflammatory claimsfor MMJ.
Factors that would most influence willing APMs’ future prescribing involve more detailed data about the medical benefits (claims) for cannabis. Data needs, in priority order include:
- Data for immunomodulating properties and the impact of cannabis on malignancies
- Data on the psychoactive properties of cannabis
- Data on the anti-inflammatory properties of cannabis
- Risks of MMJ (both short- and long-term)
Profile: APMs currently willing to recommend MMJ to their pain patients are generally comfortable with the logistics of acquiring a MMJ Card and where patients can find MMJ. This comfort with recommending MMJ is revealed in their willingness to widely discuss MMJ with their patients.
They are now seeking more data to substantiate the medical claims made for MMJ. In addition, as with all APMs, validating the safety of cannabis is paramount. While these willing APMs seemed to have had positive experiences with recommending MMJ, they recognize that their observations need to be validated by large long-term studies and endorsement from industry experts.
APMs who are unsure whether or not to recommend MMJto their pain patients have a low familiarity with cannabis topics. As such, these APMs discuss MMJ with the fewest number of patients.
Data that would most influence these APMs’ future decisions about MMJ include (in priority order):
- Pharmacologyof cannabis, in particular: CBNs, Terpenes, interactions among Terpenes-THCs-CBD, and more information on the human endocannabinoid system.
- The stance of the American Medical Association (AMA) toward MMJ
- Risks of MMJ (both short- and long-term)
Profile: APMs currently on-the-fence about whether or not to recommend MMJ in the future are the least informed about MMJ. As such, they do not have well-formed opinions (positive or negative) about cannabis. Left to their own, with 1 or 2 bad patient experiences, they could easily become unwilling to consider MMJ for their patients.
To move them into the “willing” category, on-the-fence APMs need detailed data behind the science of cannabis (e.g., pharmacology of components and how these interact with the human endocannabinoid system). In order for them to address and contextualize patient-reported side effects, these APMs also need more data on the safety of the drug.
APMs who are unwilling to recommend MMJto their pain patients seem to have had a bad experience with MMJ in the past. They have the most familiarity about the short- and long-term risks of MMJ, and they are significantly more likely than even willing APMs to discuss these issues with their patients.
Other than safety issues with MMJ, unwilling APMs have the least amount of familiarity with most other cannabis topics and have spoken with the fewest number of pain patients about nearly all MMJ topics (except for safety).
Topics that may lessen the opposition toward MMJ among these unwilling APMs include the following (in priority order):
- Risks of MMJ (both short- and long-term)
- Requirements by the State in order for a patient to get a MMJ Card
- Clinical claims of efficacy
Profile: APMs currently unwilling to recommend MMJ in the future seem to have had either a bad experience with MMJ (e.g., patients with unacceptable side effects) or have received bad information about MMJ. These APMs have more familiarity with various cannabis topics than do those APMs who are on-the-fence, but below that of willing APMs.
Despite a moderate level of familiarity with MMJ (relative to other APMs), these APMs are not only unwilling to recommend MMJ, but they discuss risks of MMJ with more patients than any other type of APM. Data needs to be shown to these unwilling APMs that demonstrates that MMJ is largely safe and that serious side effects are rare. Once this barrier is crossed, these APMs need to see data convincing them of the clinical benefits of the drug.
Conclusions
As shown in the study findings, information is key to encouraging APMs’ to recommend MMJ for their patients. Given the low level of understanding of various cannabis topics, companies looking to market to healthcare providers need to understand the current knowledge-based of targeted physicians in order to craft messaging that is most compelling to each.
Increasing confidence in MMJ by APMs will come about through educational opportunities whereby physicians can hear from reputable sources about the latest data surrounding the use of MMJ for pain. As demonstrated by the pharmaceutical industry, focusing on the education of physicians in overcoming their hesitancy and other barriers to recommending MMJ pays dividends by:
- Providing physicians (and their staff) with the logistical and clinical information they are desperately seeking but don’t have the time or bandwidth to seek this information on their own.
- Allowing physicians to more effectively guide patients and reinforce safe use of MMJ.
- Demonstrating that your company cares about patients and their health issues.
- Helping form partnerships and build trust with the MMJ industry.
1]Habib, G. and Avisar, I. The Consumption of Cannabis by Fibromyalgia Patients in Israel. Pain Research & Treatment. 2018; July 22.
[2]Russo, E.B. Cannabinoids in the management of difficult to treat pain. Therapeutics & Clinical Risk Management. V.4(1)
[3]Martin-Sanchez E, Toshiaki A., et al (2009) Systematic Review and Meta-analysis of Cannabis Treatment for Chronic Pain.Pain Medicine.
MJ Shareholders
MJShareholders.com is the largest dedicated financial network and leading corporate communications firm serving the legal cannabis industry. Our network aims to connect public marijuana companies with these focused cannabis audiences across the US and Canada that are critical for growth: Short and long term cannabis investors Active funding sources Mainstream media Business leaders Cannabis consumers









No comments so far.
Be first to leave comment below.