
Classifying Medical Cannabis vs. Traditional Pharmaceuticals Guides Marketing Efforts
Marijuana Industry NewsMedical Marijuana September 3, 2019 MJ Shareholders 0
When considering Medical Cannabinoid Therapy (MCT), most informed physicians and patients focus on two classes of cannabinoids: tetrahydrocannabinols (THC) and cannabidiols (CBD). However, research has identified over 500 compounds in cannabis, including over 120 distinct cannabinoids and over 100 terpenes. Despite this focus on the two types of cannabinoids, research into the benefits of MCT have shown that positive clinical outcomes are rarely due to a single cannabinoid or terpene. Rather, studies have shown that benefits are achieved through an interaction between multiple cannabinoids and terpenes.
Research identifying the specific combinations and terpenes that provide a specific clinical outcome is still in its infancy and, to-date, no particular strain has been discovered or engineered with a specific clinically relevant combination of cannabinoids and terpenes for treating a specific pathology. This raises the question:
How does Cannabis fit into the current structure of medicines available to consumers?
Currently, there are three major classifications for pharmaceuticals:
- Level of access to the medicine: prescription versus over-the-counter/self-help medications[i]
- Structure/Origin of molecule: synthetic versus biological
- Level of protection for innovators: branded versus generic
So, why is it important to properly classify medical cannabis and cannabinoids? Mainly, because the classification of a product in the healthcare space determines the methods by which effective promotional campaigns are created. In this review, we will examine the current regulations for each of these classifications and assess the degree to which cannabis may fit into or compare to any single category.
Level of Access:
Very simply, a prescription drug is one that requires a medical prescription by a licensed healthcare provider (typically a physician) in order to be dispensed. In contrast, an over-the-counter (OTC) drug does not require authorization from a licensed healthcare provider. Both prescription and OTC drugs must be approved by the national health regulatory agency (e.g., FDA, Health Canada, EMA) and have been tested for efficacy and safety when taken for their indicated use. For both prescription and OTC medications, the regulatory agency takes the stance that these drugs are considered unsafe until proven safe. It should be noted that OTC medicines are not the same as dietary supplements and nutraceuticals. The most important distinction is that these supplements are viewed by the FDA to be safe until proven unsafe.[ii]
In the USA, the Dietary Supplement Health and Education Act (DSHEA) of 1994 defined dietary supplements as a category of food. The DSHEA says that dietary supplements cannot contain anything that may have “a significant or unreasonable risk of illness or injury” when the supplement is used as directed on the label. “New” supplements that contain an ingredient not recognized as a food substance, must provide the FDA with reasonable evidence that the new ingredient is safe, but manufacturers are not required to test new ingredients or supplements in clinical trials, which would help find risks and potential interactions with drugs or other substances.
Requirements for Approval of Prescription and OTC Medications in the USA[iii]
|
Feature: |
Prescription Drug |
OTC Drug |
|
Uniqueness |
Must not be chemically or structurally equivalent to any other medicinal compound |
Must be chemically or structurally similar to another medicinal compound |
|
How accessed |
Prescribed by licensed healthcare provider |
No pre-authorization required |
|
How acquired |
Purchased in a pharmacy or licensed distributor (mail-order pharmacy, manufacturer) |
Purchased off-the-shelf or behind-the-counter by consumers |
|
How regulated (in USA) |
By the FDA through a New Drug Application (NDA) process |
By the FDA through OTC drug monographs |
|
How promotion is regulated (in the USA) |
All promotional claims are reviewed and monitored by the FDA |
Federal Trade Commission (FTC) has authority, just as with other consumer products |
When examining legal medical cannabis in this context, it is easily seen where the overlap and differentiation exists.
- Cannabis plants are rarely unique. As of May 2019, there are currently only 5 US plant patent cases (4 pending applications, 1 issued patent), and 11 utility plant-directed patent cases (8 pending applications, 3 issued patents).[iv] With many databases listing over 1,500 strains (phenotypes) of cannabis, plants that are shown to be unique are extremely rare.
- Access to Cannabis distribution is strictly regulated. All current Medical Cannabis legislation requires that patients interested in using MCT must be evaluated by a licensed physician to determine the existence of specific pre-existing conditions eligible for MCT. Unfortunately, few, if any, require that a patient’s attending physician sign-off on the MCT.
- Acquisition of Medical Cannabis is only made though a specialty “distributor”. In some respects, this model is closer to that of prescription drugs in that Medical Cannabis can only be obtained through licensed “pharmacies” (dispensaries) or via mail-order directly from licensed distributors/manufacturers.
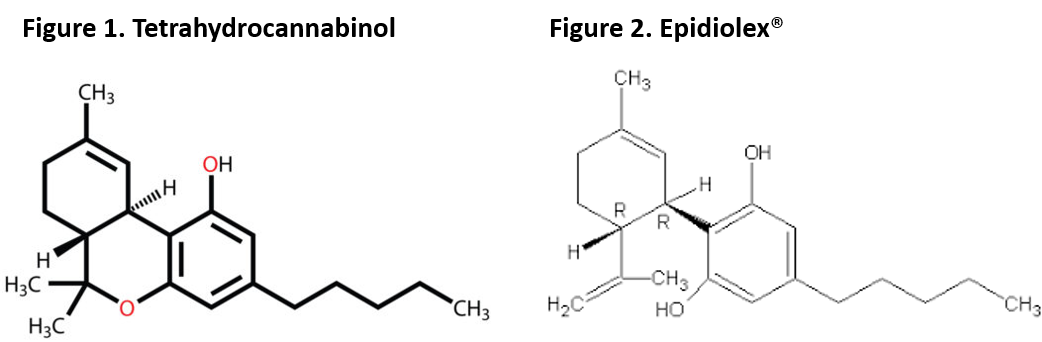
- Regulation of MCT is done at the state level in the USA. Currently, the FDA has no role in the licensing, testing, and monitoring of medical cannabis (except in the rare incidence where cannabinoids have been tested through the NDA process, e.g. Epidiolex®).
- Promotion of cannabis is limited (if allowed at all). Most states limit most promotions of cannabis products so as to NOT promote the recreational use or divert the medical cannabis. In some instances, these limits prevent signage or displays of any cannabis-related products. Further direct-to-consumer advertising is almost always banned. In addition, despite the FDA currently taking a “hands-off” approach to regulation of MCT in the USA, they have recently sent warning letters to cannabis manufactures about making medical and/or safety claims that are not supported by large-scale clinical trials.
Regarding the level in which patients have access to MCT, cannabis is more closely aligned with prescription drugs than OTC drugs. Further, it is clear that cannabis (as currently viewed by regulatory agencies) is not a nutraceutical or dietary supplement. Given the current position of the FDA, it is hard to predict how they would regulate access to MCT if assigned that charge by Congress. However, with their recent activity warning against claims and their generally conservative approach, it most likely that MCT would align more closely with prescription drugs than with OTCs.
Structure/Origin:
Drugs today fall into two major categories describing their origins – synthetic and biologic. Most medications are typically manufactured through chemical synthesis by combining specific chemical ingredients in an ordered process. Biologics, in contrast, are manufactured in a living system such as a microorganism, plant or in animal cells. Most biologics are very large, complex molecules or mixtures of molecules. In addition, instead of being manufactured through chemical synthesis, biologic products are often produced using recombinant DNA technology[v].
Synthetic drugs generally have well-defined chemical structures, and a finished drug can usually be analyzed to determine all its various components. As such, manufacturers of synthetic compounds can change the manufacturing process extensively and analyze the finished product to establish that it is the same as before any manufacturing change. By contrast, it is difficult, and sometimes impossible, to analyze the complexity of a biologic in the laboratory. Some of the components of a finished biologic may be unknown. As such, manufacturers must ensure product consistency, quality, and purity by demonstrating that the manufacturing process remains substantially the same over time. This requires that the process controls for biologics must be established separately for each unique product and are not applicable to a product created by another manufacturer. Therefore, it improbable for a second manufacturer to make the “same” biologic without intimate knowledge of and experience with the innovator’s process.
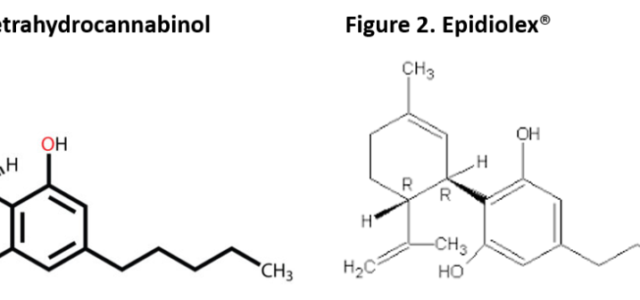
Synthetic cannabinoids such as Marinol or Syndros (dronabinol), are currently available as prescription medications in the US, Canada, and Europe. These drugs employ a single cannabinoid (synthetic tetrahydrocannabinol) and are available as both a branded and generic prescription medications.
Synthetic medications have a clear advantage over biologic medication in that physicians and patients make clear assumptions about synthetics that cannot be applied to biologics:
- Because they are manufactured in a lab, there are fewer confounds to creating a copy of the drug over and over, thus the consistency from dose to dose is consistent.
- Because the clinical properties of a synthetic drug are most often due to a single compound/molecule, it is easier to theorize about the physiological properties and mechanism of action of the drug.
Conversely, due to the complex structure of and difficult manufacturing process for a biologic medication, “certainties” such as dosing consistency and clear mechanism of action cannot be fully known. Hence, a biologic must rely more on its clinical profile whereas a synthetic can leverage their theoretical underpinnings.
Level of Protection:
The third classification for pharmaceuticals is the level of protection a drug has from being copied and marketed by competitors. The two categories are branded (protected by patent with years of market exclusivity) and generic (copies of drugs whose patent has expired).
Branded drugs are those synthetic or biologic agents that the FDA has approved for specific indications. These drugs hold patents for their chemistry/structure and for their brand (image). The manufacturer/patent-holder has market exclusivity typically for 20 years. During this timeframe, the FDA (in the USA) continues to monitor the drug for untoward side effects and the accuracy of promotional claims. As a drug nears the end of its patent, manufacturers try various techniques to preserve their patent and delay generic competition. These include, expanding the indication to different diseases or populations, providing marginal improvements to the delivery or formulation, etc.
Ultimately, at the end of a drug’s patent, competitors will begin filing their copies/versions as a generic prescription. Once the FDA deems that the originator has no claim to a patent extension, they begin to review generic applications. The only protection that a generic drug typically has is a patent on its brand (e.g., name, packaging, etc.), but not the active ingredient[vi].
The FDA requires companies to demonstrate that the generic medicine can be effectively substituted and provide the same clinical benefit as the brand-name medicine that it copies using the following requirements:
- The active ingredient in the generic medicine must be the same as in the brand-name drug/innovator drug.
- The generic medicine must have the same strength, use indications, form (such as a tablet or an injectable), and route of administration (such as oral or topical).
- The inactive ingredients of the generic medicine must be acceptable, however different.
- The generic medicine must be manufactured under the same strict standards as the brand-name medicine.
- The container in which the medicine will be shipped and sold should be appropriate, and the packaging label describing ingredients, uses, and warnings must be the same as the brand-name medicine’s label.
In some instances, the originator drug cannot be turned into a generic. This is either due to the complexity of the chemistry/manufacturing process or if the drug is a biologic medication. In the first instance, the originator usually does not face competition despite the lack of patent on the drug. In the second instance, a new class of medication has been created, call a biosimilar.
Biosimilar drugs and generic drugs are very different. Generic drugs are near identical to the original in chemical composition. Therefore, regulatory agencies state that generics are “therapeutically equivalent” to the innovator drug and are interchangeable with it iv. Conversely, biosimilar drugs are only “highly similar” in structure and chemical composition to the originator. However, they are close enough in duplication to accomplish the same therapeutic and clinical results[vii].
When a biosimilar manufacturer establishes a new manufacturing process, beginning with new starting materials, it will produce a product that is different from and not therapeutically equivalent with that of the innovator. Because of the complexity of biologics, the only way to establish whether there are differences that affect the safety and efficacy of the follow-on product is to conduct clinical trialsiv. In 2018, the FDA published its standards for approving new biosimilars. These standards included small-scale clinical trials, along with full chemical, biophysical and molecular comparisons with the originator. Without these trials, the FDA has no evidence to assume equivalency with the original biologic, and thus cannot grant it substitution rights.
Level of Market Protection
|
Branded Pharmaceutical |
Biosimilar Pharmaceutical |
Generic Pharmaceutical |
|
|
Who owns patent on active ingredients? |
Originating Manufacturer |
No one |
No one |
|
Who owns the patents on product branding? |
Originating Manufacturer |
Biosimilar Manufacturer |
Generic Manufacturer |
|
Market exclusivity |
Yes (20 yrs.) |
Yes (12-42 mon.) |
Yes (180 days for first filer) |
|
Requirement for interchangeability |
N/A |
PK/PD analysis & Clinical Trials |
Chemical Analysis |
So, into what classification does medical cannabis fit? Recall, long-term market exclusivity protection comes to the holder of the drug’s patent (i.e., chemistry/manufacturing process). Thus, insofar as the FDA is concerned, a branded medication has unique chemical and biological properties.
Two non-synthetic cannabinoid products – Epidiolex® and Sativex® – have pending patents in the US by GW Pharmaceuticals. As single, naturally occurring cannabinoids, the chemical structure of these drugs is easily understood (and published in the label). Upon patent expiration, generics can be synthesized in a similar process.
Epidiolex and Sativex filed patents due to the unique structure and manufacturing process of the single active ingredient, THC. However, the benefits derived from most strains/varieties of cannabis are attained through the interaction of natural occurring cannabinoids, terpenes and other chemicals manufactured by the plant. But, can a plant be patented?
 Under U.S. federal law, new plant varieties can be protected under the Plant Variety Protection Act (PVPA), as a plant patent under the Plant Patent Act (PPA), or as a utility patent under the Patent Act. Plant varieties could also be trade secrets or subject to contractual (licensing) protection[viii]. In December 2016, the U.S. Patent and Trademark Office has issued a plant patent for the cannabis plant ‘Ecuadorian Sativa’, and utility patents for this variety covering: breeding, production, processing, and use of specialty cannabis.
Under U.S. federal law, new plant varieties can be protected under the Plant Variety Protection Act (PVPA), as a plant patent under the Plant Patent Act (PPA), or as a utility patent under the Patent Act. Plant varieties could also be trade secrets or subject to contractual (licensing) protection[viii]. In December 2016, the U.S. Patent and Trademark Office has issued a plant patent for the cannabis plant ‘Ecuadorian Sativa’, and utility patents for this variety covering: breeding, production, processing, and use of specialty cannabis.
How Plants are Patented in the USA vi
|
Plant Variety Protection Act |
Plant Patent Act |
Utility Patent Act |
|
|
What is protected? |
Sexually reproduced plant varieties |
Asexually reproduced plant varieties |
Covers the creation of a new or improved—and useful—product, process, or machine. |
|
Requirements? |
Variety must be new, distinct, uniform, and stable, accordingly to USDA regulations. |
Variety must be new, nonobvious, and have some significant utility. Plant must differ from known plants by at least one distinguishing characteristic (more than that caused by different growing conditions or fertility). |
Plants, seeds, plant varieties, plant parts, and processes of producing plants, plant genes, and hybrids. Variety must be new, nonobvious, and have some utility, among other things. |
|
Limitations? |
Plant patent has only a single claim that defines the scope of the patent. |
Limited to one genome of the plant. Mutations or hybrids would not be covered in the patent but could be separately patentable. |
More stringent requirements for applications than plant patents, but generally offer broader protections than plant patents. Can have multiple claims, each addressing different parts of the plant or ways of using the plant. |
|
Duration? |
20 years |
20 years |
20 years |
The vast majority of medicinal cannabis plants available today are grown through asexual reproduction (e.g., cloning). As shown in multiple studies, one of the current problems faced by MCT is consistency of product and outcomes from dose-to-dose and from prescription-to-prescription. Cloning provides a means for assuring more consistent crops.
“Cloning is crucial for [cannabis] growers looking for consistency in their genetics,” says veteran grower Allie Beckett, author of As the Grass Grows. “Seeds may be more vigorous growth-wise, but they are often unreliable in terms of phenotypes [physiological traits]. Cloning guarantees the preservation of your genetics — it can be a finicky process, but it is absolutely a necessary one.[ix]”
The difference between a plant generated by sexual reproduction and a plant generated by cloning is a significant issue in the MCT market today. The most common approach in identifying the medical benefits of a particular strain is to examine the results of ingestion. If this results in a positive outcome, the strain is deemed “appropriate” for a condition or symptom. While somewhat effective for identifying “classes” of strains (e.g., heady-high, body-high, relaxing, invigorating, etc.) it does not: 1) identify the specific cannabinoids, terpenes or other chemicals leading to positive outcomes, 2) identify the specific cannabinoids, terpenes or other chemicals having no physiological impact or leading to side effects, 3) determine the specific combinations or interactions of cannabinoids, terpenes or other chemicals that lead to an optimal benefit while minimizing risks/side effects.
The process of genetically modifying cannabis plants is in its infancy, although in June 2019, Trait Biosciences, Inc. developed the first-ever successful stable genetic transformation of the Cannabis Sativa plant. This process has been given a Plant Variety Patent for breakthrough technology platforms that produce truly water-soluble cannabinoids and dramatically increase cannabinoid yields in hemp and cannabis[x]. This opens the door for researchers to develop other genetically modified strains that more closely target the physiological mechanisms associated with various disease processes and reduces the risk of adverse events.
Implications of Classifying Medical Cannabis on Marketing Efforts
Recall, that the classification of a product in the healthcare space determines the methods by which effective promotional campaigns are created. Promotions of pharmaceuticals typically cover two issues – promoting the product and promoting the brand. Understanding and articulating the difference to your customer base is crucial to success.
The status of the MCT product being promoted helps define the parameters of a promotional campaign. Knowing the expectations of healthcare providers for specific types of medications allows manufacturers to focus their efforts and avoid confusing claims.
So, how do the various classifications for cannabis impact the promotional process?
Prescription versus OTC status: Currently medical cannabis straddles the line between Rx and OTC. Only one cannabis strain is available today that can claim that they are “not chemically or structurally equivalent to any other medicinal compound” as other prescription drugs. However, individual cannabinoids (e.g., Epidiolex) can demonstrate this uniqueness. Further, MCT can only be accessed through physician consent (albeit recreational users can attain cannabis and use it for medical purposes) in specialized, licensed, distribution facilities (e.g., dispensaries). To-date both the FDA and Health Canada appear to view cannabis as a prescription drug requiring controls to access and distribution.
Implications: Promotion of a prescription medication requires involving the healthcare community, especially physicians, in the conversations. OTC drugs do not require physician pre-authorization; hence, marketing efforts can be solely focused on the patient.
Synthetic versus Biological: The vast majority of cannabis-based products are biologic in nature in that manufacturers use plants as grown either in the form of flower or by extracting the naturally occurring cannabinoids and terpenes that correlate with a clinical benefit. While synthetic cannabinoids have be created in the laboratory (e.g., Marinol), science has been slow to genetically modify cannabis plants in order to create new species. This is largely due to the unknown mechanisms by which individual cannabinoids effect the body. As more is learned about the specific physiological impact and interactions of cannabinoids on various disorders, scientists will undoubtedly begin developing breeds of plants that concentrate target cannabinoids (in specific combinations and ratios) and eliminate other chemicals that may interfere with the effectiveness of the plant or increase a patient’s risk factors.
Implications: Promotion of biologic medications is much more complex that the promotion of synthetics. This difficulty involves the inability of biologic manufactures to play upon the natural assumptions of physicians and patients about synthetic drugs. Where a synthetic manufacturer can rely on a drug’s molecular structure and manufacturing techniques to assure consistency and safety, a biologic manufacturer must rely solely on the clinical picture presented by their drug, while still addressing concerns about consistency and safety.
Branded, Biosimilar or Generic: Recall, that for a medicinal product to be branded, the manufacturer must hold patents for the drug’s chemistry/structure and the brand (image). To-date, the only unique cannabis plant that has been patented is the one engineered by Cannabis Sativa, Inc. (see above). All other cannabis plants are hybrids shared among producers. Cannabis plants can also not be considered generics. Generics are copies of branded drugs whose patent has expired. Cannabis products available on the market today are most similar to biosimilars. Unlike generics, biosimilars cannot be automatically substituted. Rather, biosimilar drugs are only “highly similar” in accomplishing the same therapeutic and clinical results as others.
Implications: Promotion of biosimilars is much different from traditional branded pharmaceuticals. For biosimilars, the manufacturer must convince end-users that 1) the drug/plant has the same clinical effectsas others in terms of safety and efficacy, but 2) the manufacturer has branded the drug with specific features to enhance the overall experience of end-users.
[i] In Canada, OTC drugs are often referred to as Self-Care Medications.
[ii] https://www.cancer.org/treatment/treatments-and-side-effects/complementary-and-alternative-medicine/dietary-supplements/fda-regulations.html
[iii] https://www.fda.gov/drugs/questions-answers/prescription-drugs-and-over-counter-otc-drugs-questions-and-answers
[iv] https://www.forbes.com/sites/julieweed/2017/07/24/us-patent-office-issuing-cannabis-patents-to-a-growing-market/#34cb842268d4
[v] https://www.bio.org/articles/how-do-drugs-and-biologics-differ
[vi] Note: the first generic company to market has a 180-day market exclusivity period before another generic can enter the market.
[vii] https://www.cancercenter.com/community/blog/2018/12/whats-the-difference-biosimilar-and-generic-drugs
[viii] https://www.cannalawblog.com/cannabis-patents-the-101/
[ix] http://www.pbs.org/independentlens/blog/growing-industry-weed-seeds-giving-way-pot-clones/
[x] https://www.biospace.com/article/releases/trait-biosciences-secures-breakthrough-patents-for-truly-water-soluble-cannabinoids/
MJ Shareholders
MJShareholders.com is the largest dedicated financial network and leading corporate communications firm serving the legal cannabis industry. Our network aims to connect public marijuana companies with these focused cannabis audiences across the US and Canada that are critical for growth: Short and long term cannabis investors Active funding sources Mainstream media Business leaders Cannabis consumers








No comments so far.
Be first to leave comment below.