
Legal Implications for Physicians Recommending Medical Cannabis in the USA
Marijuana Industry NewsMedical Marijuana July 18, 2019 MJ Shareholders 0
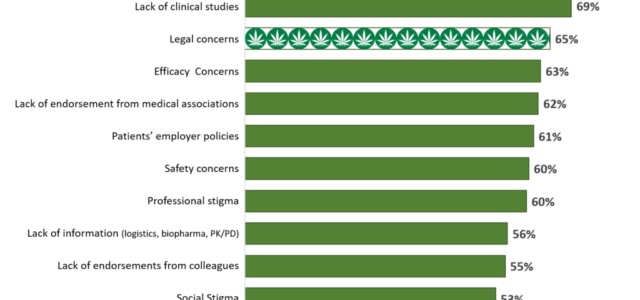
In our studies examining the use of Medical Cannabis Therapy (MCT) by Oncologists and Pain Management Specialists[i], we asked physicians what their biggest barrier was to their adoption of medical cannabis. Two-thirds (65%), mention legal concerns. Concern for legal exposure and increased risk of malpractice associated with MCT remains high, given the federal status of cannabis being Schedule I.
To contextualize the degree in which legal concerns have on physicians’ behavior, it is second only to the lack of clinical trials in preventing physicians from recommending MCT to patients. In addition, lack of reliable guidance (from medical associations or colleagues), concern that patients will be punished by their employer, and professional/social stigma of being known as a MCT endorser are also significant barriers to adoption of cannabis into their treatment armamentarium.

However, this raises the question: What are the actual legal risks to physicians if recommending MCT as a treatment for their patients?
Based on federal regulations, if a physician was to prescribe MCT it would constitute aiding and abetting the acquisition of marijuana, which could result in revocation of DEA licensure and even prison time. However, in states where medicinal cannabis is legal, doctors can write a recommendation for the plant, after determining and certifying that the patient suffers from one of the conditions that the state’s law deems to warrant medicinal cannabis. This recommendation “loophole” was upheld by the US Court of Appeals for the Ninth Circuit in Conant v. Walters, which decided that a physician’s discussion of the potential benefits of medicinal cannabis and making such recommendations constitute protected speech under the First Amendment. The court reasoned that doctors should not be held liable for conduct that patients might engage in after leaving the office and that open and unrestricted communication is vital in preserving the patient-doctor relationship and ensuring proper treatment[ii],[iii],[iv].
Amended AMA Policy:
Patients also face legal jeopardy through their employers. Both state and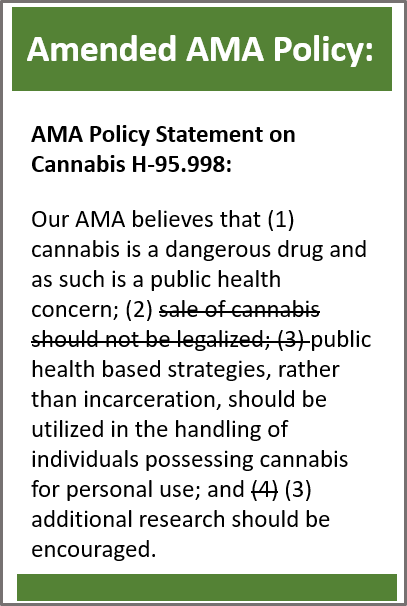 federal courts have upheld firing an employee for medical cannabis use. Employees have been unsuccessful when challenging employee statutes, citing state medical cannabis laws as well as federal and state anti-discrimination laws to justify their MCT. The state medical cannabis laws ordinarily immunize medical cannabis users from the adverse consequences of the law, but do not give them a right that can be used affirmatively against a private entity. The Americans with Disabilities Act (ADA) and similar state anti-discrimination in employment statutes are predicated upon discrimination based on lawful activity and the Controlled Substances Act has consequently proven to be an insurmountable obstacle iIi.
federal courts have upheld firing an employee for medical cannabis use. Employees have been unsuccessful when challenging employee statutes, citing state medical cannabis laws as well as federal and state anti-discrimination laws to justify their MCT. The state medical cannabis laws ordinarily immunize medical cannabis users from the adverse consequences of the law, but do not give them a right that can be used affirmatively against a private entity. The Americans with Disabilities Act (ADA) and similar state anti-discrimination in employment statutes are predicated upon discrimination based on lawful activity and the Controlled Substances Act has consequently proven to be an insurmountable obstacle iIi.
Finally, medical associations within the USA are cautiously developing guidelines for use and monitoring of cannabinoids. Most advocate individualized approach to cannabinoid recommendations/use, with careful monitoring of beneficial and adverse effects. The American Medical Association has been advocating for the re-scheduling of cannabis in order to facilitated large, well-controlled clinical trials of cannabinoids. Yet, they have been slow to modify their published recommendations about MCT.
But, isn’t recommending MCT the same as off-label use of approved pharmaceuticals?
The FDA makes it clear that it does not regulate the practice of medicine and that the federal Food, Drug, and Cosmetic Act of 1938 will not play a role in creating physician liability for off-label drug use [v]. Before using a drug off-label, physicians are trained to ask themselves five questions [vi]:
- Does the drug have FDA approval?
- Has the off-label use been subjected to substantial peer review?
- Is the off-label use medically necessary for treatment?
- Is the use of the medication nonexperimental?
- Am I using this off-label drug in good faith, in the best interest of the patient, and without fraudulent intent?
It is not necessary for a physician to answer in the affirmative to each of these questions in order to prescribe a drug off-label. However, the further they stray, the more legal jeopardy they place themselves into.
So, why not just have a patient sign a consent form to lessen the physician’s liability?
To-date, no court has mandated that a physician must disclose, through an informed consent process, the off-label use of a drug. In fact, informed consents may unintentionally bias a patient by 1) unduly frightening patients, and 2) placing a burden on physicians forcing them to constantly review and communicate medication risk and benefit information. This may divert attention away from other more important patient care issues [vii]. Further, a case in 1972, stated: the test for determining whether a particular peril must be divulged is its materiality to the patient’s decision.” A material risk is one in which “a reasonable person, in what the physician knows or should know to be the patient’s position, would be likely to attach significance to the risk or cluster of risks in deciding whether or not to forego the proposed therapy.[viii]
MCT, while somewhat supported by off-label use practices, remains apart from traditional pharmaceuticals due to its Schedule I status. While opioids account for roughly 25% of drug-related medical malpractice lawsuits in the US[ix], to-date, no court has considered potential malpractice liability for a physician certifying or recommending medical cannabis. Courts may, however, be expected to confront such cases as more states approve the use of MCT and as substantially more patients gain access to cannabis. If wide-spread use begins to uncover serious health risks, there continues to be a lack of evidence supporting the use of MCT for a variety of health conditions, and with less risky FDA approved pharmaceutical cannabinoids continue to enter the market, legal risk of recommending MCT may grow. Douglas Marlowe, JD/PhD[x], former Chief of Science, Law & Policy for the National Association of Drug Courts and Associate Professor of Psychiatry at the University of Pennsylvania Medical School, outlines the process most likely to be taken by the courts when a malpractice suit involving the use of MCT eventually is filed.
First the courts will need to address whether certifying the need for medical cannabis creates a traditional doctor/patient relationship. This carries with it a concomitant duty to render competent professional care. A professional duty of care is created by the virtue of the powers and authority vested in physicians through state licensure and accreditation laws, as well as the reasonable expectations of patients. If a patient is legally obligated to obtain certification for medical cannabis from a physician, and if the patient reasonably believes that the physician will exercise professional judgment and training in making that decision, then a doctor/patient relationship is likely to be recognized. Courts typically find that a doctor/patient relationship has been created where the physician assumed some degree of responsibility for making a diagnostic or treatment decision or saw the patient as part of a formal consultation even if the physician had no further involvement with the patient’s care.
The second issue involves the courts determining whether a physician has breached the duty of care by engaging in substandard medical practice. For example:
- Did the physician breach the duty of care by failing to take an adequate medical history of a patient which would have uncovered contraindicated conditions that are likely to be made worse by cannabis use?
- Did a physician breach the duty of care by certifying cannabis to treat a condition that is unlikely to improve from its use.
Some states employ a custom-based test for determining the standard of carex, requiring the physician to provide the type and level of care that an ordinary and prudent physician with comparable training and experience would have provided under similar circumstances in the same or a similar locality. In these states, expert testimony from physicians who are familiar with the relevant locality and area of practice is usually required to establish the customary standard of care.
In contrast, a growing number of states apply a reasonable physician standardx, which evaluates the physician’s actions against what he or she should have done as opposed to what is customarily done. In these states, expert witnesses may describe the results of
scientific studies to support their conclusions about reasonable care, or on cross-examination, may be called upon to defend their conclusions in the face of conflicting findings.
So how does a conscientious physician recommend MCT while minimizing their legal liability?
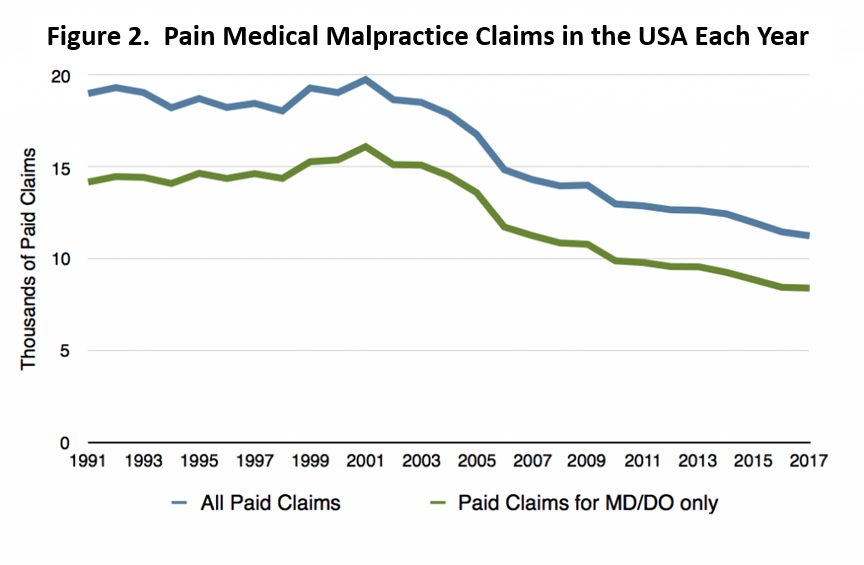
Although the number of medical malpractice claims has been dropping since 2001, nearly 8,500 claims were filed against physicians in the US in 2018[xi].
In order to minimize the legal jeopardy of physicians, the Federation of State Medical Boards has provided guidelines for practitioners considering the use of MCT for their patients [xii].
- Assure that a collaborative effort has been established between physician and patient. The physician-patient relationship is fundamental to the provision of acceptable medical care. Therefore, physicians must have documented that an appropriate physician-patient relationship has been established, prior to providing a recommendation, attestation, or authorization for MCT to the patient. Failing to obtain adequate informed consent from patients may expose physicians to third-party liability for foreseeable harms to other persons. For example, physicians could be held liable to third parties who are injured in a car or work accident caused by a patient’s use of cannabis. Although the physician has no doctor/patient relationship with the third parties, s/he may be liable in ordinary negligence for nonfeasance by failing to take simple precautions that could have avoided a serious injury. Courts have found physicians liable to third parties for failing to warn patients about potential driving hazards associated with the use of prescription medications. Warning a patient about risks associated with MCT is ordinarily sufficient to shield the physician from third-party liability even if the patient ignores the physician’s advice and engages in hazardous activity. Courts will typically view a patient’s willful noncompliance with a physician’s directive as an intervening factor that erases a physician’s legal liabilityix.
- Document the patient medical evaluation and relevant clinical history. At minimum, the evaluation should include the patient’s history of present illness, social history, past medical and surgical history, alcohol and substance use history, family history with emphasis on addiction or mental illness/psychotic disorders, physical exam, documentation of therapies with inadequate response, and diagnosis requiring the MCT recommendation.
- Provide the patient with information about the known and unknown risk/benefits of MCT. Patients should be advised of the variability and lack of standardization of cannabis preparations and the known effects of cannabis. Patients should be reminded not to drive or operate heavy machinery while under the influence of cannabis. Most states apply an objective test for causality of malpractice. This requires that an ordinary, reasonable and prudent patient would not have undergone the treatment if the potential harms had been disclosed. Other states apply a subjective test that requires that the patient would have elected to proceed with a treatment in light of the known medical risks and benefits. Therefore, it is incumbent upon a physician to disclose all known risk of MCT to the patient.
- Develop a written treatment plan agreed upon by the patient. A written treatment plan that includes:
- Review of other attempts to ease the suffering caused by the medical condition that do not involve the recommendation of cannabinoids.
- Advice about other options for managing the condition.
- Determination that a terminal or debilitating medical condition may benefit from MCT.
- Advice about the potential risks of the medical use of cannabis.
- Additional diagnostic evaluations or other planned treatments.
- A specific duration for the MCT for a period no longer than twelve months.
- A specific ongoing treatment plan as medically appropriate.
- Verify qualifying conditions. Recommending cannabis for certain medical conditions is at the professional discretion of the physician. The indication, appropriateness, and safety of the recommendation should be evaluated in accordance with current standards of practice and in compliance with state laws, rules and regulations which specify qualifying conditions for which a patient may qualify for MCT.
- On-going monitoring and adaptions to the treatment plan. The physician should regularly assess the patient’s response to the use of cannabis and overall health and level of function. This assessment should include the efficacy of the treatment to the patient, the goals of the treatment, and the progress of those goals.
- Consult and refer patients with a history of substance abuse or mental health disorders. A patient who has a history of substance use disorder or a concomitant mental health disorder may be at a higher risk than others using cannabis. As such, these patients should be referred to a pain management specialist, psychiatrist, or to an addiction/mental health specialist.
- Maintain accurate and complete medical records. Keep accurate and complete medical records, and should include but not necessarily limited to:
- The patient’s complete medical history
- Results of the physical examination, patient evaluation, diagnostic, therapeutic, and laboratory results
- Other treatments and prescribed medications
- Authorization, attestation or recommendation for MCT (include date, expiration, and any additional information required by state statute)
- Instructions to the patient, including discussions of risks and benefits, side effects and variable effects
- Results of ongoing assessment and monitoring of patient’s response to MCT
- A copy of the signed Treatment Agreement, including instructions on safekeeping and not diverting.
- Eliminate conflicts of interest between physician and cannabis supply. Do not have a professional office located at a dispensary or cultivation center or receive financial compensation from or hold a financial interest in a dispensary or cultivation center. Nor should the physician be a director, officer, member, incorporator, agent, employee, or retailer of a dispensary or cultivation center.
In conclusion, a mindful physician has little to be concerned about regarding the recommendations of MCT to their patients as long as they apply sound medical practices to their use of cannabis. Maintaining accurate and thorough records of the interaction between themselves and patients, provides the physicians with a wide degree of authority by the courts to assess and determine the best therapeutic interventions for the patients. By becoming educated about the latest scientific data and opinions about the benefits, risks, and mechanism of action for medical cannabis, a physician can inoculate themselves against legal issues.
[i]Clinical realities of MMJ for Pain in the USA: Cannalytic Insights, October 2018. https://cannalyticinsights.com/mmjinsights/ and Clinical Realities of MMJ for Cancer in the USA: Cannalytic Insights, October 2018. https://cannalyticinsights.com/mmjinsights/.
[ii]Gregorio, J. Physicians, Medical Marijuana, and the Law. AMA Journal of Ethics. Sept. 2014.
[iii]Garvey, T., Doyle, C. and Carpenter, D.H., Marijuana: Medical and Retail – Selected Legal Issues. Congressional Research Service. April 8, 2015. 7-5700.
[iv]Conant v Walter, 309 F3d 629, 636 (9th Cir 2002)
[v]Bax Global Inc v Brenneman, Ohio 695 (Ohio Ct App 2007).
[vi]Committee on Drugs, American Academy of Pediatrics Uses of drugs not described in the package insert (off-label uses) Pediatrics. 2002;110(1):181–183.
[vii]Wilkes M., Johns M. Informed consent and shared decision-making: a requirement to disclose to patients off-label prescriptions. PLoS Med. 2008;5(11):1553–1556.
[viii]Canterbury v Spence, 464 F2d 772 (DC Cir 1972).
[ix]Opioid epidemic leads to increase in medical malpractice claims, civil lawsuits. Spangenberg, Shibley & Liber, LLP.
[x]Marlowe, D.B. Malpractice Liability and Medical Marijuana. The Health Lawyer. American Bar Association Health Law Section. Vol. 29; Num. 2. Dec. 2016.
[xi]Beck, D., MD. The True Cost of Health-care: Malpractice Statistics. http://truecostofhealthcare.org/malpractice_statistics/
[xii]Model Guidelines for the Recommendation of Marijuana in Patient Care. Report of the FSMB Workgroup on Marijuana and Medical Regulation. Adopted as policy by the Federation of State Medical Boards. April 2016
MJ Shareholders
MJShareholders.com is the largest dedicated financial network and leading corporate communications firm serving the legal cannabis industry. Our network aims to connect public marijuana companies with these focused cannabis audiences across the US and Canada that are critical for growth: Short and long term cannabis investors Active funding sources Mainstream media Business leaders Cannabis consumers








No comments so far.
Be first to leave comment below.